Psychiatric Clinical Co-Pilots: The Ethical Response to Cognitive Overload in Modern Psychiatry
Psychiatry has always carried a distinct moral weight.
Few medical specialties require clinicians to make decisions that simultaneously affect biological function, psychological identity, social stability, and personal autonomy. Diagnosis is rarely binary. Risk is rarely fully measurable. Treatment decisions often unfold over time, influencing the trajectory of a person’s life in ways that extend far beyond symptom relief.
Yet modern psychiatric practice is changing, not because the science is failing, but because the cognitive demands of practice are expanding faster than clinicians’ capacity to manage them safely.
Today’s psychiatrist is expected to synthesize evolving diagnostic frameworks, increasingly complex psychopharmacology, risk assessment obligations, regulatory documentation, medical comorbidity considerations, and fragmented longitudinal histories, often within time-pressured clinical environments.
This growing complexity has introduced a new ethical question:
Is it still responsible to expect clinicians to manage high-stakes psychiatric decision-making without structured cognitive support?
This question has given rise to a new concept in modern care: the psychiatric clinical co-pilot.

Psychiatric Clinical Co-Pilot and the Cognitive Crisis in Psychiatry
Psychiatry is fundamentally a reasoning-intensive discipline. Unlike procedural specialties that rely heavily on instrumentation, psychiatric decision-making depends on probabilistic thinking, pattern recognition, longitudinal synthesis, and contextual judgment.
In a single clinical encounter, a psychiatrist may need to:
Formulate a diagnosis based on incomplete or evolving data
Evaluate cumulative medication risks across multiple systems
Assess suicide or violence risk with limited objective markers
Decide between admission, observation, or outpatient management
Translate complex reasoning into defensible documentation
Each step introduces uncertainty. When combined, they create significant cognitive load, particularly in emergency, inpatient, consultation-liaison, and crisis stabilization settings.
Research increasingly suggests that errors in psychiatry are rarely caused by lack of knowledge. Instead, they often emerge from fragmented reasoning, time pressure, and cognitive overload.
This burden contributes to broader physician burnout trends. Surveys have shown that over 60% of physicians report symptoms of burnout, with mental health specialties consistently ranking among those experiencing high emotional exhaustion and administrative strain. The expansion of documentation demands alone has been identified as a major contributor to clinician fatigue.
Against this backdrop, the psychiatric clinical co-pilot is not being proposed as a technological novelty. It is emerging as cognitive infrastructure, a way to stabilize reasoning quality under real-world conditions.
Psychiatric Clinical Co-Pilot vs the Fear of Replaced Judgment
One of the most persistent ethical concerns surrounding the psychiatric clinical co-pilot is the fear that clinical judgment will be outsourced.
This concern is legitimate. Ethical psychiatric care requires that diagnosis, risk formulation, treatment planning, and disposition decisions remain the responsibility of a trained clinician capable of interpreting nuance and consequence.
However, support does not inherently imply substitution.
Psychiatrists have long relied on structured aids, diagnostic criteria, medication algorithms, supervision, case conferences, and clinical checklists. These tools were never intended to replace judgment; they were designed to anchor reasoning during complexity.
What has changed is not the philosophy of support, but the volume and fragmentation of information clinicians must manage simultaneously.
Modern psychiatric clinical co-pilot systems aim to organize clinical thinking at the moment it is occurring, surfacing considerations, highlighting risks, and structuring logic without dictating conclusions.
In this model, the clinician remains the pilot. The system assists with navigation.

Psychiatric Clinical Co-Pilot and Ethical Responsibility
Another concern frequently raised is the risk of responsibility diffusion. If structured decision support contributes to clinical reasoning, where does accountability reside?
In psychiatry, the answer must remain unequivocal.
Responsibility cannot drift. It must remain entirely with the treating clinician.
Well-designed psychiatric clinical co-pilot models emphasize clinician-in-the-loop architecture as an ethical safeguard rather than a technical feature. The clinician authors the note, signs orders, determines the diagnosis, and owns the outcomes.
Decision support in this context is not about shielding responsibility; it is about clarifying reasoning. Many psychiatrists describe these systems as functioning like a highly structured second set of eyes, particularly useful in high-pressure environments where cognitive bandwidth is limited.
Transparency of reasoning can strengthen ethical practice by making assumptions visible rather than implicit.
Psychiatric Clinical Co-Pilot as Cognitive Infrastructure; Not Automation
Across medicine and other high-reliability fields such as aviation and critical care, structured cognitive support has become standard practice. Checklists, monitoring frameworks, and decision pathways exist not to replace expertise but to reduce variability driven by fatigue or overload.
Psychiatry’s reliance on nuanced judgment may make it particularly suited to thoughtful co-pilot models.
Variability in symptom presentation, increasing polypharmacy complexity, medico-legal exposure related to risk assessment, and the growing involvement of non-psychiatrists in mental health care all contribute to decision density.
When reasoning is made explicit, when alternatives are surfaced and safety factors highlighted, clinicians may be better positioned to apply judgment consistently.
In this sense, the psychiatric clinical co-pilot can function as an ethical prompt, encouraging reflection rather than enforcing pathways.

Psychiatric Clinical Co-Pilot and Documentation as an Ethical Act
Documentation in psychiatry is not merely administrative. It is an ethical artifact, a record of how risk was weighed, autonomy respected, and treatment decisions justified.
When documentation is delayed or reconstructed after the fact, ethical clarity can erode. Memory biases, time pressure, and narrative compression may distort the reasoning that actually occurred.
Structured documentation support offered by psychiatric clinical co-pilot systems allows clinicians to capture clinical thinking while the encounter is still fresh. This approach does not embellish decisions; it preserves them.
Clear documentation can improve continuity of care, strengthen medico-legal defensibility, and reduce the cognitive burden of after-hours charting, factors closely linked to burnout.
Psychiatric Clinical Co-Pilot in Education and Workforce Stability
The implications of cognitive support extend beyond individual clinicians to the future psychiatric workforce.
Psychiatry faces persistent shortages globally. At the same time, trainees often encounter wide variability in supervision exposure, diagnostic rigor, and prescribing confidence.
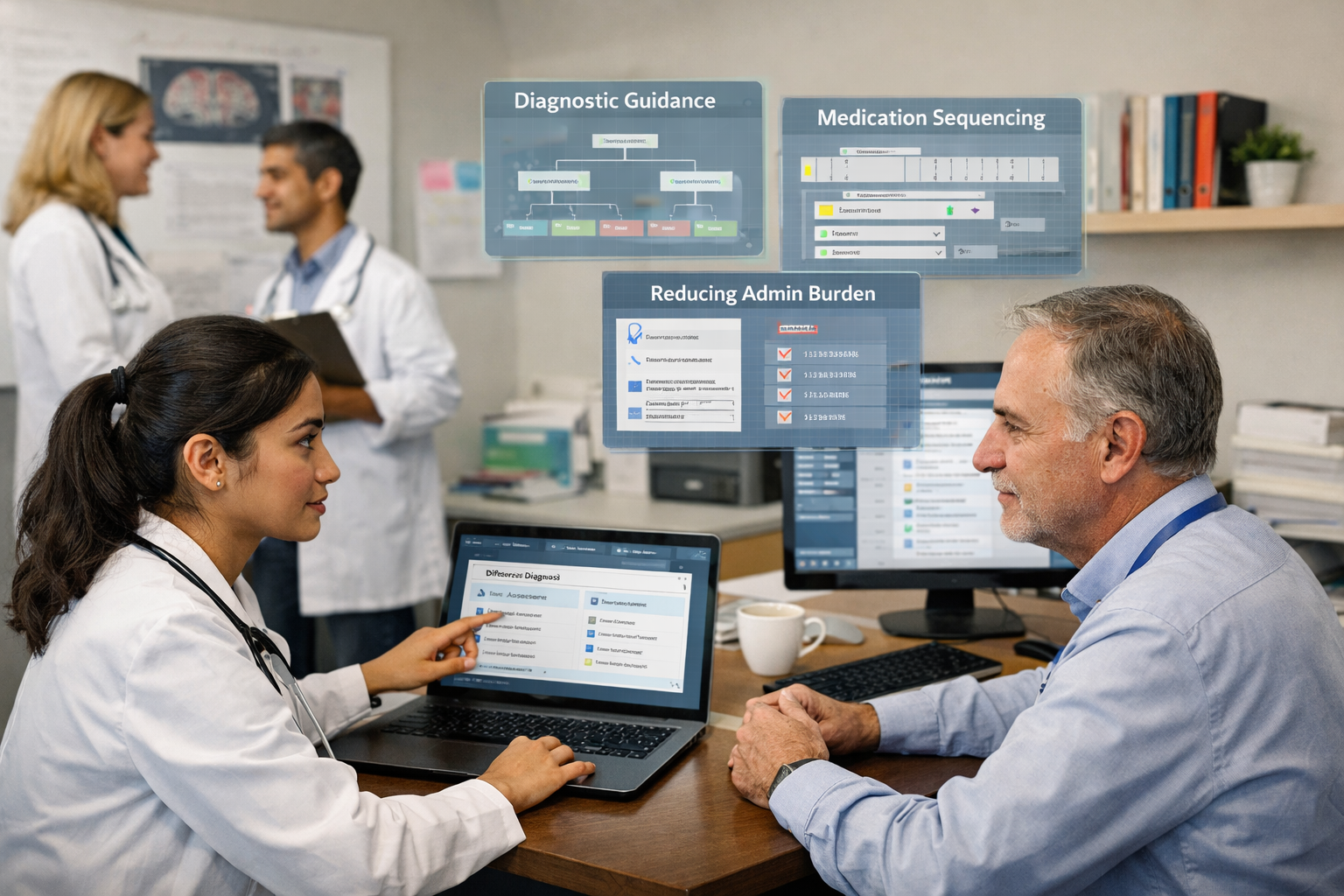
Structured reasoning support can function as scaffolding, helping learners develop frameworks for differential diagnosis, risk assessment, and medication sequencing while maintaining faculty oversight.
Experienced clinicians may also benefit. Surveys suggest that administrative load and decision fatigue contribute significantly to early retirement and reduced clinical hours. Tools that stabilize workflow and reduce cognitive friction may therefore play a role in workforce sustainability.
On-Demand Psychiatry: A Real-World Psychiatric Clinical Co-Pilot
Among emerging platforms, On-Demand Psychiatry represents a psychiatry-specific clinical co-pilot model developed from real-world clinical workflows.
Designed with clinician-in-the-loop principles, the platform aims to support structured reasoning during diagnostic formulation, medication safety review, risk assessment, and documentation. Rather than generating autonomous treatment decisions, it is intended to organize complexity so that clinicians can apply their judgment more clearly.
This distinction is critical.
On-Demand Psychiatry reflects a broader shift in the field, from viewing decision support as a potential threat to autonomy toward understanding it as infrastructure for safe thinking under pressure.
By aligning with the realities of modern practice, fragmented histories, regulatory demands, and high-risk prescribing environments, psychiatry-specific co-pilot systems may help clinicians preserve both accountability and therapeutic presence.

Frequently Asked Questions
Does a psychiatric clinical co-pilot replace professional judgment?
No. When designed responsibly, it supports reasoning without dictating decisions. The clinician remains fully accountable.
Is this ethically different from traditional guidelines?
Yes. Guidelines are static references. Clinical co-pilots provide contextual support at the point of care with clinician oversight.
Why are experienced psychiatrists using these systems?
Often to manage complexity, maintain consistency, reduce cognitive load, and improve documentation clarity, not due to lack of knowledge.
Where does On-Demand Psychiatry fit within this landscape?
It is an example of a clinician-built psychiatric clinical co-pilot designed to align with real-world workflows while preserving autonomy and responsibility.
Closing Reflection: The Future of Thoughtful Psychiatry
Ethical psychiatry has never been about rejecting tools. It has always been about choosing tools that respect human judgment.
As clinical complexity continues to grow, the central challenge may not be whether clinicians should use structured cognitive support, but how to use it without compromising accountability, empathy, or individualized care.
The future of psychiatry is unlikely to be fully manual, nor fully automated.
It will be collaborative.
It will be deliberate.
It will remain clinician-led.
And in an era defined by cognitive overload, the psychiatric clinical co-pilot may represent not a departure from ethical practice, but a necessary evolution of it.